The Process Of Cultural Competemility
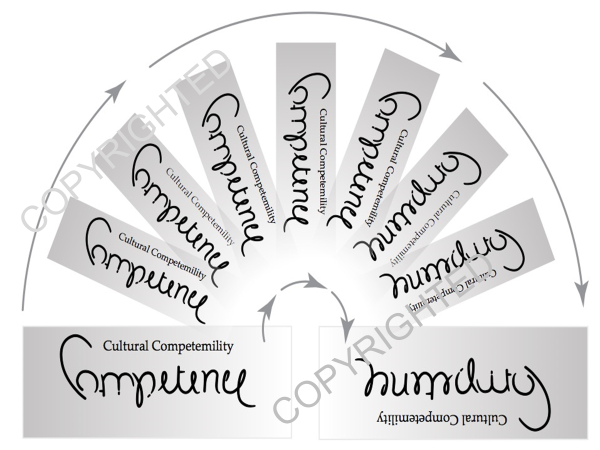
The Process of Cultural Competemility in the Delivery of Healthcare Services model asserts that cultural humility and cultural competence must enter into a synergistic relationship, resulting in a combined effect that is greater than the sum of their separate effects. This synergistic relationship is embodied in the term, “cultural competemility.” The origin of cultural competemility is the deliberate blending of the terms cultural competence (compete) and cultural humility (mility) to create the coined term cultural competemility. Cultural competemility is defined as the synergistic process between cultural humility and cultural competence in which cultural humility permeates the five components of cultural competence: cultural awareness, cultural knowledge, cultural skill, cultural desire, and cultural encounters. The result of this total permeation of cultural humility into cultural competence can be symbolically represented in a rotating ambigram. An ambigram is a word, art form, or other symbolic representation whose elements retain meaning when viewed or interpreted from a different direction, perspective, or orientation. The below figure displays an ambigram in which the word competence, when rotated clockwise, spells the word humility. Thus, humility is found in competence and competence is found is humility.
To fully grasp the model, each of its construct will be defined. Cultural humility is defined as a dynamic and lifelong process focusing on self-reflection and personal critique (Tervalon and Murray-Garcia, 1998). Cultural awareness is the process of conducting a self-examination of one’s own biases towards other cultures and the in-depth exploration of one’s cultural and professional background. Cultural awareness also involves being aware of the existence of documented racism and other “isms” in healthcare delivery. Cultural knowledge is defined as the process in which the healthcare professional seeks and obtains a sound educational base about culturally diverse groups. In acquiring this knowledge, healthcare professionals must focus on the integration of three specific issues: health-related beliefs practices and cultural values; disease incidence and prevalence (Lavizzo-Mourey, 1996). Cultural skill is the ability to collect culturally relevant data regarding the patient's presenting problem, as well as accurately performing a culturally-based physical, spiritual, psychological, and medication assessments in a culturally sensitive manner. Cultural encounters is the process which encourages the healthcare professional to directly engage in face-to-face cultural interactions and other types of encounters with clients from culturally diverse backgrounds in order to modify existing beliefs about a cultural group and to prevent possible stereotyping. Cultural encounters is the pivotal construct of cultural competence that provides the energy source and foundation for one’s journey towards cultural competence. Cultural desire is the motivation of the healthcare professional to “want to” engage in the process of becoming culturally aware, culturally knowledgeable, culturally skillful and seeking cultural encounters; not the “have to.”
In summary, the Process of Cultural Competemility in the Delivery of Healthcare Services model views cultural humility, cultural awareness, cultural knowledge, cultural skill, cultural encounters and cultural desire as the essential components of cultural competemility with cultural encounters being the pivotal construct of this model. This model begins and ends with the seeking and experiencing of many cultural encounters. It is only through the infusion of cultural humility into continuous cultural encounters that one acquires cultural awareness, cultural knowledge, cultural skill and cultural desire. From this perspective, cultural competemility can be viewed as an ongoing journey of unremitting encounters.
As we begin, continue, or enhance our journey towards cultural competemility, we must humbly address the question, “Have I ASKED myself the right questions?” The following mnemonic, “A-S-K-E-D,” represents the self-examination questions regarding one’s cultural awareness, cultural skill, cultural knowledge,cultural encounters and cultural desire.
Awareness: Am I aware of my prejudices and biases, as well as the presence of racism and other ‘isms?’
Skill: Do I know how to conduct a culturally specific history, physical, mental health, medication and spiritual assessment in a culturally sensitive manner?
Knowledge: Do I have knowledge regarding different cultures’ worldview, the field of biocultural ecology and the importance of addressing social determinants of health?
Encounters: Do I have sacred and unremitting encounters with people from cultures different from mine and am I committed to resolving cross-cultural conflicts?
Desire: Do I really ‘want to’ engage in the process of competemility?
Although the above mnemonic can assist healthcare professionals in informally assessing their level of cultural competemility, healthcare professionals may want to formally assess their level of cultural competence. For this purpose Dr. Campinha-Bacote developed the tools, Inventory For Assessing The Process of Cultural Competence Among Healthcare Professionals – Revised (IAPCC-R) and Inventory For Assessing The Process of Cultural Competence Among Healthcare Professionals – Student Version (IAPCC-SV). These tools are based on her model of cultural competence and have sound psychometric properties. Please refer to the website links on the IAPCC-R (link) and IAPCC-SV (link) for more information regarding these tools.
Development Of The Model (1991-2018)
The following comments reflect the development of Campinha-Bacote’s model, The Process of Cultural Competemility in the Delivery of Healthcare Services. For more detailed information about the model please refer to the publication, The Process of Cultural Competemility in the Delivery of Healthcare Services: Unremitting Encounters, 6th edition (2020) at https://transculturalcare.net/books-2/). If you are interested in purchasing a copy of this book, refer to the following link at https://transculturalcare.net/order-form/.
1991 - The development of my current model of cultural competemility has been an ongoing process of almost 30 years. This process began in 1991 when I conceptualized and named the model, “Culturally Competent Model Of Care.” In this first version, I identified four constructs of cultural competence: cultural awareness, cultural knowledge, cultural skill, and cultural encounters (figure 1, below).
1998 - In 1998 I revised my initial conceptualization of the model for the constructs were very limited in scope and needed to be expanded to include new knowledge in the field of transcultural health care, and the pictorial representation of this model appeared linear. The first version of the model did not clearly depict cultural competence as a “process” and the pictorial representation did not express the interdependent relationship between the constructs. I also felt that cultural competence was more than just awareness, knowledge, skill and encounters. Therefore, in the second revision I added a fifth construct called cultural desire, modified the pictorial representation of the model as a Venn diagram to reflect the interdependent relationship between the five constructs, and expanded the definitions of the constructs of cultural awareness, cultural knowledge and cultural skill (figure 2, below). I renamed the model, “The Process of Cultural Competence in the Delivery of Healthcare Services,” to reinforce that it was a process.
2002 - In 2002, the key role that cultural desire played in the process of becoming culturally competence became evident, yielding further revision of the model’s pictorial representation. I enhanced the model to symbolically represent a volcano. In this pictorial revision, cultural desire was identified as the construct that ignited the process of becoming culturally competent. (figure 3, below).
2010 - In 2010, I began collecting evidenced-based research studies using my model and tool (IAPCC-R), and discovered that the pivotal and key construct in the process of becoming culturally competent was cultural encounters. With this added research-base knowledge I amended the pictorial representation to focus and center around the construct of cultural encounter (figure 4 below). This model begins and ends with the seeking and experiencing of many cultural encounters and it is only through continuous cultural encounters that one acquires cultural awareness, cultural knowledge, cultural skill and cultural desire.
2018 - In 2018, the final revision of The Process of Cultural Competence in the Delivery of Healthcare Services model (figure 5 below) involved three changes: 1) the infusion of cultural humility into the five constructs of cultural competence; 2) a linguistic change from the term cultural competence to the term cultural competemility; and 3) the model’s name change to,“The Process of Cultural Competemility in the Delivery of Healthcare Services”. These revisions were based on concepts of my model, “A Biblically Based Model of Cultural Competence in the Delivery of Healthcare Services” as well as the ongoing debates centering around the relationship between the concepts of cultural competence and cultural humility.
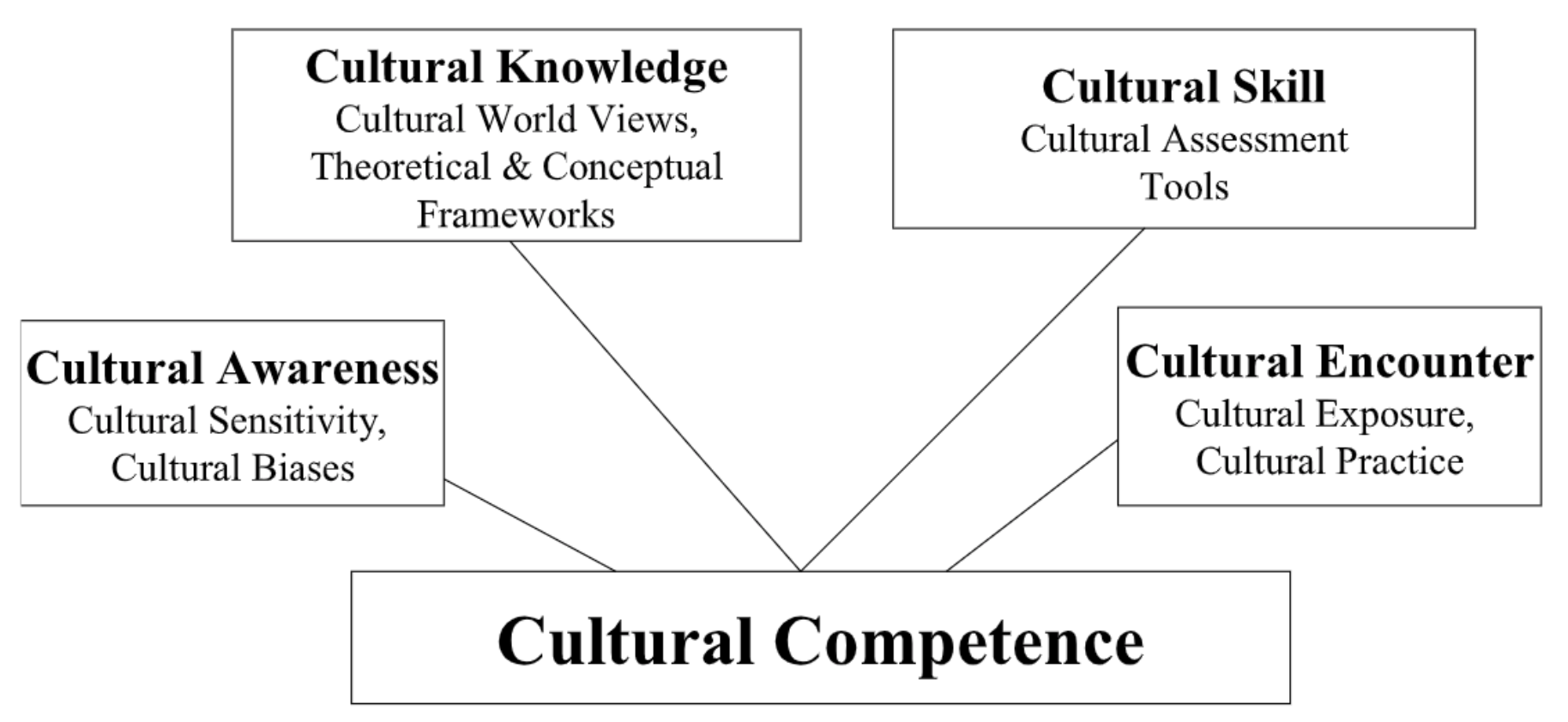
Figure 1
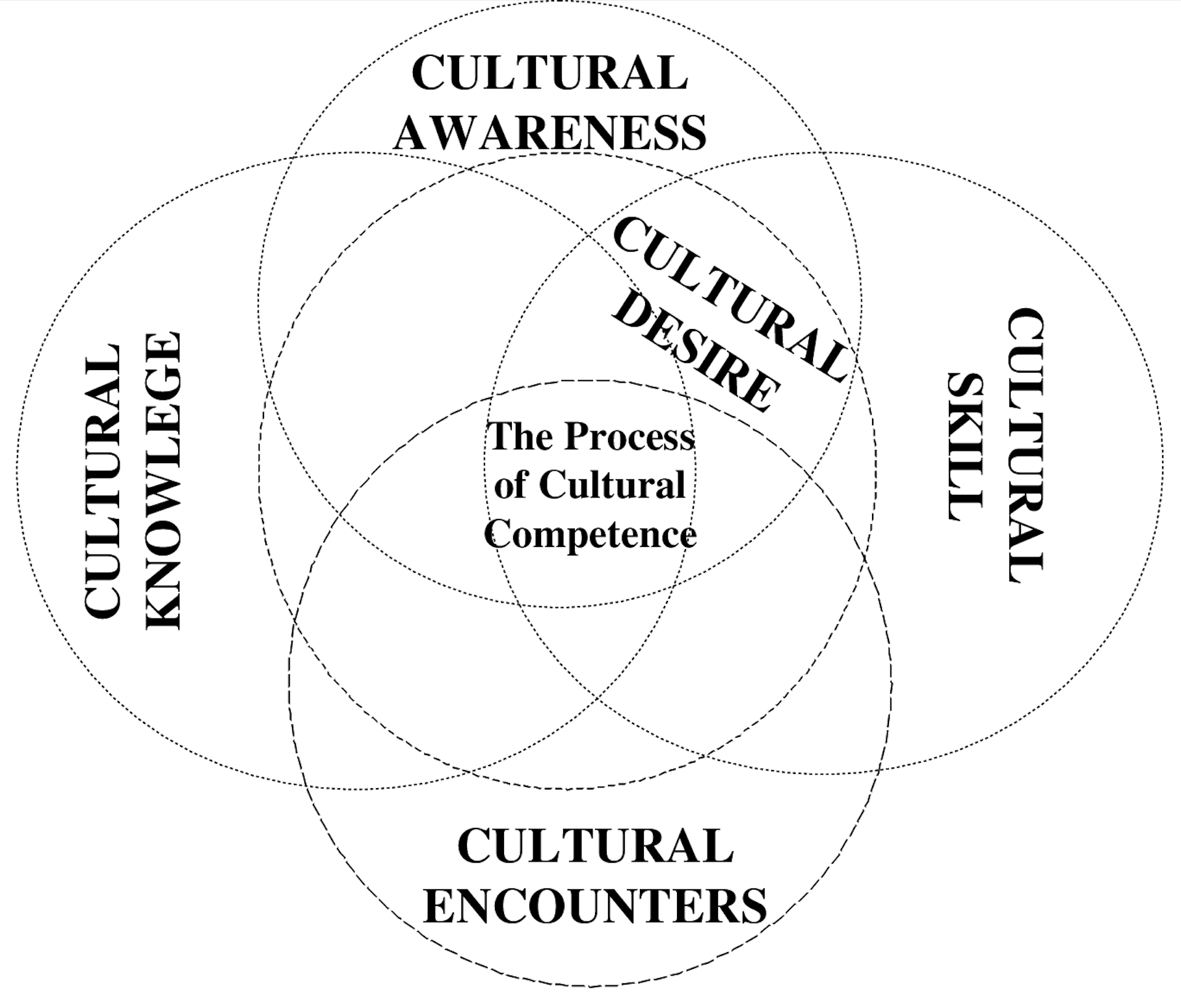
Figure 2
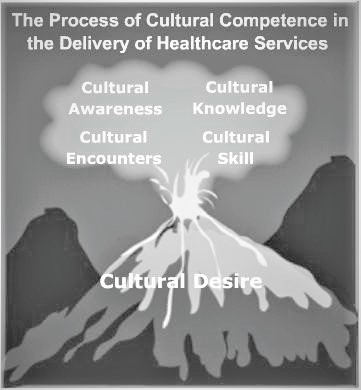
Figure 3
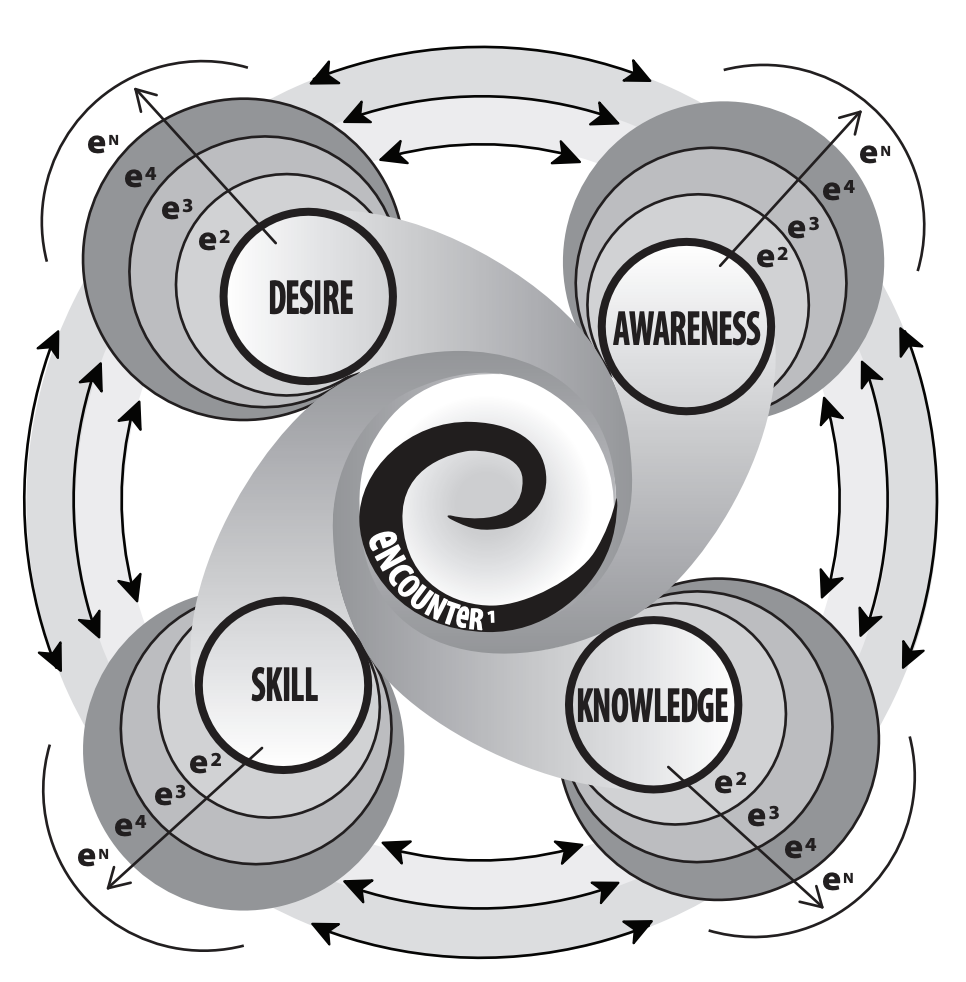
Figure 4
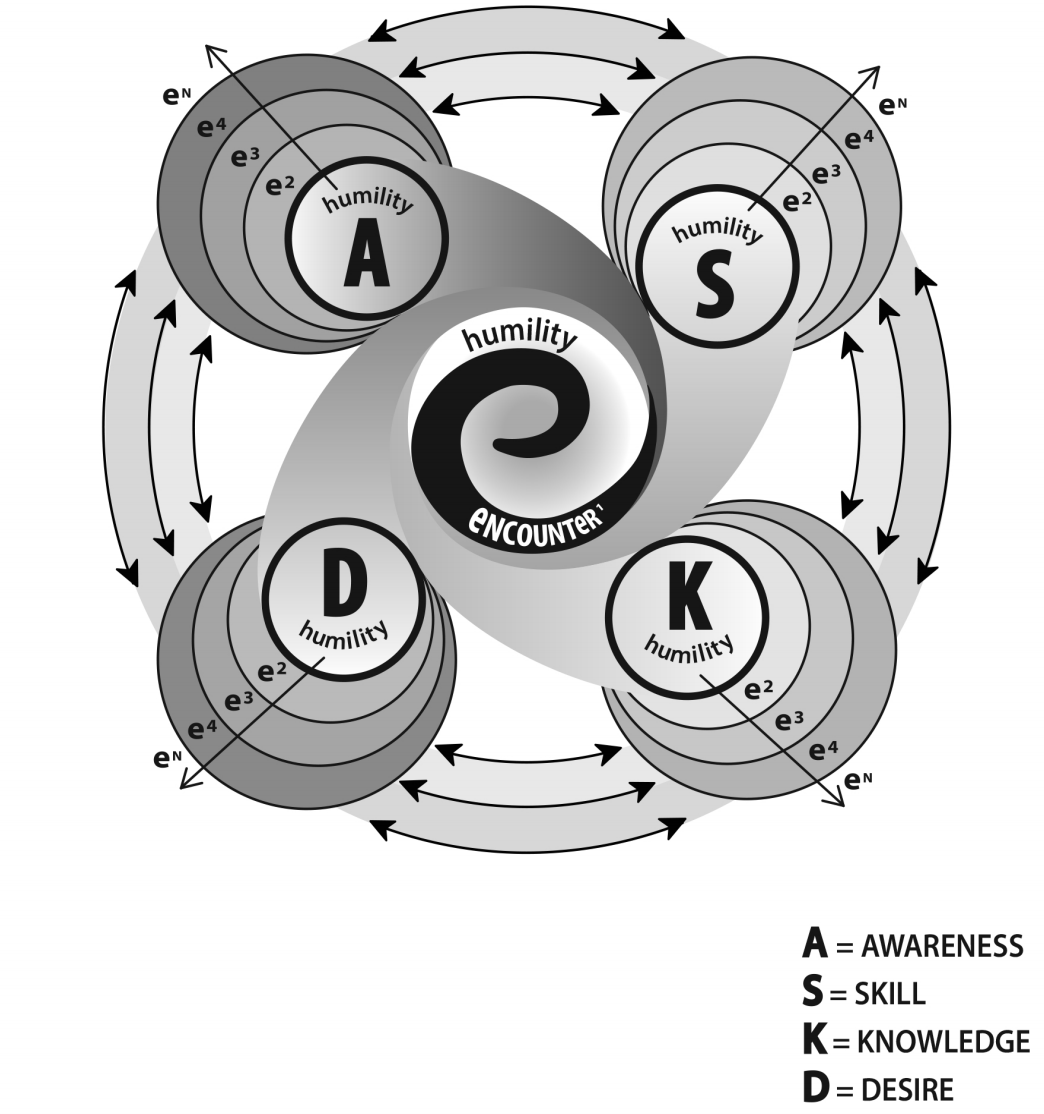
Figure 5
The Process of Cultural Competemility in the Delivery of Healthcare Services
©Copyrighted by Campinha-Bacote (2018); not to be reprinted without permission
Please note that all ambigram, graphic, pictorial, and mnemonic figures displayed on this web page are copyrighted and cannot be reprinted without formal written permission from Transcultural C.A.R.E. Associates. Thank you for your understanding of the intellectual property and legal copyright status of these models.